1. Correction
Following the release of the "Integrated Household Survey, January to December 2013" statistical bulletin, an error was found in the section for "Perceived General Health by Occupation". This error related to the following paragraph:
"Adults in Routine and Manual Occupations (12.6%) were more likely to consider themselves ‘not in good health’ compared with adults in Intermediate (17.8%) or Managerial and Professional (21.7%) Occupations (Figure 7)."
This paragraph should have read:
"Adults in Routine and Manual Occupations (21.7%) were more likely to consider themselves ‘not in good health’ compared with adults in Intermediate (17.8%) or Managerial and Professional (12.6%) Occupations (Figure 7)."
This error only affected the text in the bulletin. Figure 7 and the underlying data in the bulletin remain unchanged.
ONS apologises for any inconvenience this may have caused.
Back to table of contents2. Main findings
In 2013, 1.6% of UK adults identified their sexual identity as gay, lesbian or bisexual
London had the highest percentage of adults identifying themselves as gay, lesbian or bisexual at 3.2%
Twice as many males (1.6%) as females (0.8%) were likely to state their sexual identity as gay or lesbian
Smoking prevalence in the UK fell from 19.8% in 2012 to 18.7% in 2013
Smoking prevalence was substantially lower in females (16.5%) than in males (21.1%). A similar pattern emerged for every age group
More males perceived their general health as good (77.1%) than females (74.8%). A similar pattern emerged for every age group
3. Introduction
This bulletin provides information from the January to December 2013 Integrated Household Survey (IHS).
The IHS is the largest social survey collected by the Office for National Statistics (ONS). It provides estimates from approximately 340,000 individual respondents - the biggest pool of UK social survey data aside from the census.
The IHS has been developed by ONS to be a cost-effective way of obtaining a large dataset with a number of topics. It also enables analysis at lower level geographies that cannot typically be obtained with other social surveys. The IHS is used by academics, government departments, and other stakeholders to provide evidence for planning, policy and monitoring purposes. It specifically provides data on sexual identity, smoking prevalence and perceived general health to meet users’ needs.
This large sample size is achieved by asking a core suite of questions on two ONS household surveys: the Annual Population Survey (APS) and the Living Costs and Food Survey (LCF). More detailed information on the survey, and how to carry out your own analyses, can be found in the background notes.
Following a statistical products consultation in 2014, the LCF will no longer form part of the IHS from 2014. This means this will be the last release of the IHS based on cases from the APS and LCF. Future releases will be based solely on the APS.
At present, IHS statistics are designated as experimental. Information on what this means can be found in the background notes.
This release provides estimates from data collected in the UK between January and December 2013. Readers interested in previous IHS releases can find these on the IHS release page.
Back to table of contents4. Sexual identity
The Integrated Household Survey (IHS) asks a question on self perceived sexual identity of adults in the UK. This question was developed as part of the ONS Sexual Identity Project, which developed, tested and implemented the question to satisfy the increasing demand for data on sexual orientation to meet 2010 Equality Act1. ONS focussed on one component of sexual orientation, sexual identity, as this is the most relevant dimension of sexual orientation to investigate given its relation to experiences of disadvantage and discrimination.
In 2013, the Integrated Household Survey found 1.6% of adults identified themselves as either gay, lesbian or bisexual2. This comprised of:
1.2% of adults identified themselves as gay or lesbian
0.5% of adults identified themselves as bisexual
This compares with 1.5% of adults who identified themselves as gay, lesbian or bisexual in 2012, which represents a small increase in 2013. This difference was not, however, statistically significant3.
Sexual Identity by Gender
Males were twice as likely as females to consider themselves gay or lesbian:
1.6% of adult males identified themselves as gay or lesbian compared to 0.8% of adult females
Adult females were more likely to identify themselves as bisexual (0.6%) compared to adult males (0.4%)
Table 1 summarises the distribution between sexual identity and gender in 2013.
Table 1: Sexual Identity: by Gender, UK, January to December 2013
| % | |||
| Gender | 2013 | ||
| Men | Women | Total | |
| Heterosexual / Straight | 92.3 | 93.1 | 92.7 |
| Gay / Lesbian | 1.6 | 0.8 | 1.2 |
| Bisexual | 0.4 | 0.6 | 0.5 |
| Other | 0.3 | 0.3 | 0.3 |
| Don't know / Refusal | 3.9 | 3.9 | 3.9 |
| No response2 | 1.6 | 1.4 | 1.5 |
| Source: Integrated Household Survey - Office for National Statistics | |||
| Notes: | |||
| 1. In 2013 there were 178,820 eligible respondents (aged 16 and over) to the sexual identity question. Of these, 169,102 provided a valid response. The question was not asked by proxy. | |||
| 2. ONS defines 'no response' as no data provided to the question by an eligible responder. A background note explains the sources of non-response to this question, the impact this has on the estimates, and ways to account for it. | |||
| 3. The 'no response' category includes respondents who were aged 15 in their wave 1 of the LFS/APS but are now aged 16 in the January to December 2013 field period. | |||
| 4. Percentages might not add to 100 per cent due to rounding. | |||
| 5. Confidence intervals for the latest estimates in the above table can be found in the Excel download table. Information on what confidence intervals are is in the background notes. | |||
Download this table Table 1: Sexual Identity: by Gender, UK, January to December 2013
.xls (30.2 kB)Sexual Identity by Region
In 2013, London had the highest proportion of adults who said they were gay, lesbian or bisexual (3.2%). The proportions of adults identifying themselves as gay, lesbian or bisexual within other regions ranged from 1.1% in the North East to 1.8% in the North West. Differences between these other regions were not, however, statistically significant (as shown by the confidence intervals displayed in Figure 1).
Figure 1: Sexual Identity: by UK Region, January to December 2013
Source: Integrated Household Survey - Office for National Statistics
Notes:
- In 2013 there were 178,820 eligible respondents (aged 16 and over) to the sexual identity question. Of these 169,102 provided a valid response. The question was not asked by proxy.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are can be found in the background notes.
- The 'no response' category includes respondents who were aged 15 in wave 1 of the LFS/APS but are now aged 16 in the January to December 2013 field period. Information on a change affecting the processing of these cases can be found in the background notes.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are can be found in the background notes.
Download this chart Figure 1: Sexual Identity: by UK Region, January to December 2013
Image .csv .xlsSexual Identity by Age Group
The proportion of adults identifying themselves as gay, lesbian or bisexual in 2013 reduced through the age groups. This ranged from 2.7% of adults aged 16 to 24 who identified themselves as gay, lesbian or bisexual, to 0.5% of those aged 65 and over (Table 2). A similar pattern was found in 2012.
Table 2: Sexual Identity: by Age Group, UK, January to December 2013
| % | ||||||
| Age groups | 16-24 | 25-34 | 35-49 | 50-64 | 65+ | Total |
| Heterosexual / Straight | 89.3 | 91.6 | 92.4 | 94.2 | 94.6 | 92.7 |
| Gay / Lesbian | 1.6 | 1.8 | 1.5 | 0.9 | 0.3 | 1.2 |
| Bisexual | 1.1 | 0.6 | 0.4 | 0.3 | 0.2 | 0.5 |
| Other | 0.2 | 0.2 | 0.2 | 0.3 | 0.3 | 0.3 |
| Don't know / Refusal | 4.4 | 4.1 | 3.9 | 3.2 | 4.1 | 3.9 |
| No response2 | 3.4 | 1.7 | 1.5 | 1.1 | 0.4 | 1.5 |
| Source: Integrated Household Survey - Office for National Statistics | ||||||
| Notes: | ||||||
| 1. In 2013 there were 178,820 eligible respondents (aged 16 and over) to the sexual identity question. Of these 169,102 provided a valid response. The question was not asked by proxy. | ||||||
| 2. ONS defines 'no response' as no data provided to the question by an eligible responder. A background note explains the sources of non-response to this question, the impact this has on the estimates, and ways to account for it. | ||||||
| 3. The 'no response' category includes respondents who were aged 15 in wave 1 of the LFS/APS but are now aged 16 in the January to December 2013 field period. | ||||||
| 4. Percentages might not add to 100 per cent due to rounding. | ||||||
| 5. Confidence intervals for the latest estimates in the above table can be found in the Excel download table. Information on what confidence intervals are can be found in the background notes. | ||||||
Download this table Table 2: Sexual Identity: by Age Group, UK, January to December 2013
.xls (27.6 kB)Sexual Identity by Occupation
Adults in Managerial and Professional Occupations were more likely to identify themselves as gay, lesbian or bisexual (2.2%) compared with those in either Intermediate Occupations or Routine and Manual Occupations (1.4% for both).
Figure 2: Sexual Identity: by Occupation, UK, January to December 2013
Source: Figure 2: Sexual Identity: by Occupation, UK, January to December 2013
Notes:
- In 2013 there were 119,049 eligible respondents (aged 16 and over) to the sexual identity and occupation questions. Of these 112,604 provided a valid response. The question was not asked by proxy.
- Confidence intervals for the latest estimates in the above table can be found in the Excel download table.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are can be found in the background notes.
Download this chart Figure 2: Sexual Identity: by Occupation, UK, January to December 2013
Image .csv .xlsNotes for sexual identity
- Although the 2010 Equalities Act referred to sexual orientation, the ONS project’s question development focussed on sexual identity i.e. how people see themselves at the time the interview takes place
- This is not the sum of the two component parts due to rounding
- Information on the term ‘statistically significant’ is in the background notes
5. Smoking Prevalence
The IHS collects information on smoking prevalence rates in the UK, focussing on use of tobacco-based cigarettes by adults aged 18 and over1. This information is a key measure for monitoring tobacco use in the UK, with various initiatives in England, Wales, Scotland and Northern Ireland launched since 2011 aimed at reducing tobacco use.
The smoking prevalence rate in the UK was 18.7% in 2013. This represents a significant drop from 19.8% in 2012. Figure 3 shows the changes in smoking prevalence in all the constituent countries of the UK. The only statistically significant change came in England with the rate falling from 19.5% in 2012 to 18.4% in 2013.
ONS also collects smoking data on the Opinions and Lifestyle Survey, which has published smoking trends across Great Britain since the turn of the century. The next release of smoking data from the Opinions and Lifestyle Survey is November 2014.
Figure 3: Smoking Prevalence: by Country
January to December 2013
Source: Integrated Household Survey - Office for National Statistics
Notes:
- The total number of eligible responders to the question was 268,102 in 2013 and 264,416 in 2012. The question was asked to respondents aged 18 and over.
- Percentages may not add to 100 per cent due to rounding.
- Confidence intervals for the latest estimates in the above table are in the Excel download table. Information on what confidence intervals are is in the background notes.
Download this chart Figure 3: Smoking Prevalence: by Country
Image .csv .xlsSmoking Prevalence by Region
Regional differences in rates of smoking prevalence were found in 2013 (Table 3):
of the constituent countries of the UK, Scotland reported the highest proportion of current smokers (21.1%). England had the lowest proportion of current smokers (18.4%)2
at the regional level there appeared to be a North/South divide. Smoking prevalence in London, the South East and the South West was significantly lower than the North East, the North West and Yorkshire and The Humber
Table 3: Smoking Prevalence: by UK Region, January to December 2013
| % | |||
| Current Smoker | Ex- Smoker | Never Smoked | |
| England | 18.4 | 33.4 | 48.1 |
| North East | 22.3 | 33.0 | 44.8 |
| North West | 20.1 | 32.4 | 47.5 |
| Yorkshire and The Humber | 20.3 | 33.7 | 45.9 |
| East Midlands | 19.1 | 32.4 | 48.5 |
| West Midlands | 17.8 | 30.0 | 52.2 |
| East of England | 17.5 | 35.9 | 46.6 |
| London | 17.3 | 28.9 | 53.7 |
| South East | 17.2 | 36.5 | 46.3 |
| South West | 17.3 | 38.2 | 44.5 |
| Wales | 19.8 | 33.8 | 46.3 |
| Scotland | 21.1 | 32.4 | 46.5 |
| Northern Ireland | 18.7 | 21.3 | 60.0 |
| UK | 18.7 | 33.0 | 48.2 |
| Source: Integrated Household Survey - Office for National Statistics | |||
| Notes: | |||
| 1. The total number of eligible responders to the question was 268,102. The question was asked to respondents aged 18 and over. | |||
| 2. Percentages may not add to 100 per cent due to rounding. | |||
| 3. Confidence intervals for the latest estimates in the above table can be found in the excel download table. Information on what confidence intervals are can be found in the background notes. | |||
Download this table Table 3: Smoking Prevalence: by UK Region, January to December 2013
.xls (29.7 kB)Smoking Prevalence by Gender
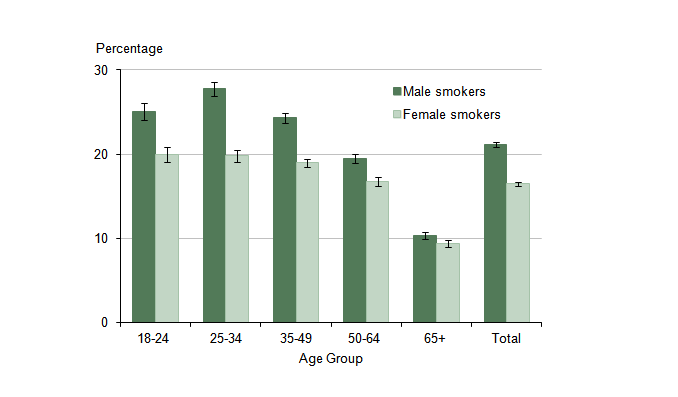
Figure 4 shows that males were more likely to be current smokers than females across every age group. This difference between males and females was more noticeable in adults aged 18-49 years old, with the gap narrowing for adults aged 50 and older. The greatest difference was in the 25-34 age group, where 27.8% of males smoked compared to 19.8% of females.
Figure 4: Current Smoking Prevalence: by Age and Gender, UK, January to December 2013
Source: Integrated Household Survey - Office for National Statistics
Notes:
- The total number of eligible responders to the question was 268,102. The question was asked to respondents aged 18 and over.
- Confidence intervals for the latest estimates in the above table are in the Excel download table.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are is in the background notes.
Download this image Figure 4: Current Smoking Prevalence: by Age and Gender, UK, January to December 2013
.png (13.6 kB) .xls (45.1 kB){kind=link}
Smoking Prevalence by Occupation3
Smoking prevalence rates also differed by occupation. Figure 5 shows 28.9% of adults in Routine and Manual Occupations were current smokers. This compared to 12.7% of adults in Managerial and Professional Occupations.
Figure 5: Current Smoking Prevalence: by Occupation, UK, January to December 2013
Source: Integrated Household Survey - Office for National Statistics
Notes:
- The total number of eligible responders to the smoking and occupation questions was 172,138. The smoking question was asked to respondents aged 18 and over.
- Confidence intervals for the latest estimates in the above table can be found in the Excel download table.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are can be found in the background notes.
Download this chart Figure 5: Current Smoking Prevalence: by Occupation, UK, January to December 2013
Image .csv .xlsNotes for smoking prevalence
- The IHS does not collect information on e-cigarettes.
- This was not significantly different to Northern Ireland who had a smoking rate of 18.7%.
- ONS has done further work looking into how differing levels of deprivation link to smoking prevalence.
6. Perceived General Health
ONS collects information on perceived general health to identify the number of adults who perceive themselves as in good health. Perceived General Health is a good predictor of demands for health services and is used in the construction of health expectancy metrics such as Healthy Life Expectancy. This provides a valuable picture of people’s perception of their general health by region, age, sex and other components.
Across the UK 75.9% of the adult population stated that they were ‘in good general health’ in 2013. This is similar to 2012 (76.1%).
Perceived General Health by Region
Regional differences were seen in UK adults’ perceptions of their general health (Figure 6):
of the constituent countries of the UK, Wales reported the lowest rate of perceived good health in 2013 (72.5%). England had the highest (76.2%)
at the regional level the North East reported the lowest rate of perceived good health (70.9%). The South East reported the highest rate of perceived good heath (78.8%) although this is not statistically significant
Figure 6: Health: by UK Region
January to December 2013
Source: Source: Integrated Household Survey - Office for National Statistics
Notes:
- The total number of eligible responders to the question was 276,522.The question was asked to respondents aged 16 and over.
- The health categories were split using the approach applied by Eurostat. 'In good health' contains the 'very good' and 'good' perceived health categories, and 'Not in good health' contains the categories 'fair', 'bad' and 'very bad'.
- Percentages may not add to 100 per cent due to rounding.
- Confidence intervals for the latest estimates in the above chart are in the Excel download table. Information on what confidence intervals are is in the background notes.
Download this chart Figure 6: Health: by UK Region
Image .csv .xlsPerceived General Health by Age and Gender
A higher proportion of men reported themselves to be ‘in good health’ compared to women. This was the case for every age group, with the biggest difference being 2.1%1 for the 35-49 years old age group.
The proportion of adults who reported themselves as ‘not in good health’ increased with age:
one in ten (10.0%) of those aged 16 to 24 considered themselves as ‘not in good health’
more than four in ten (42.4%) of those aged 65 and over considered themselves as ‘not in good health’ (Table 4)
Table 4: Health: by Age Group by Gender, UK, January to December 2013
| % | ||||||
| In good health | Not in good health | |||||
| Male | Female | Total | Male | Female | Total | |
| 16-24 | 92.3 | 90.1 | 91.2 | 7.7 | 9.9 | 8.8 |
| 25-34 | 89.3 | 87.7 | 88.5 | 10.7 | 12.3 | 11.5 |
| 35-49 | 82.4 | 80.1 | 81.3 | 17.6 | 19.9 | 18.7 |
| 50-64 | 70.3 | 70.2 | 70.3 | 29.7 | 29.8 | 29.7 |
| 65+ | 57.3 | 55.8 | 56.5 | 42.7 | 44.2 | 43.5 |
| Total | 77.7 | 75.3 | 76.5 | 22.3 | 24.7 | 23.5 |
| Source: Office for National Statistics | ||||||
| Notes: | ||||||
| 1. The total number of eligible responders to the question was 281,795 of which 281,694 provided a valid response. The question was asked to respondents aged 16 and over. | ||||||
| 2. The health categories were dichotomised using the approach applied by Eurostat. The category 'In good health' comprises the 'very good' and 'good' percieved health categories; the category 'Not in good health' comprises the categories 'fair', 'bad' and 'very bad'. | ||||||
| 3. Percentages may not add to 100 per cent due to rounding. | ||||||
| 4. Confidence intervals for the latest estimates in the above table can be found in the excel download table. | ||||||
Download this table Table 4: Health: by Age Group by Gender, UK, January to December 2013
.xls (26.6 kB)Perceived General Health by Occupation
Adults in Routine and Manual Occupations (21.7%) were more likely to consider themselves ‘not in good health’ compared with adults in Intermediate (17.8%) or Managerial and Professional (12.6%) Occupations (Figure 7).
Figure 7: Not in Good Health: by Occupation, UK, January to December 2013
Source: Integrated Household Survey - Office for National Statistics
Notes:
- The total number of eligible responders to the health and occupation questions was 172,561. The question was asked to respondents aged 16 and over.
- The health categories were split using the approach applied by Eurostat. 'In good health' contains the 'very good' and 'good' perceived health categories, and 'Not in good health' contains the categories 'fair', 'bad' and 'very bad'.
- Confidence intervals for the latest estimates in the above chart can be found in the Excel download table.
- The whisker bar represents the confidence intervals for each estimate. Information on what confidence intervals are can be found in the background notes.
Download this chart Figure 7: Not in Good Health: by Occupation, UK, January to December 2013
Image .csv .xlsNotes for perceived general health
- This difference is based on unrounded estimates and maybe different to Table 4.
7. Perceived General Health and Smoking Prevalence
When comparing smoking prevalence and general health, current smokers were less likely to report themselves to be in good health compared to those who have never smoked (Table 5).
The age of adults appeared to have an impact on the perceived general health of current smokers and non-smokers. For adults aged 18-24 years old, 81.8% of current smokers considered themselves to be in good health. This is compared with 91.9% who had never smoked; a difference of 10.2%1.
For adults aged 50-64 years old, the difference was larger. Of current smokers, 56.7% considered themselves in good health. This compared with 75.9% of adults who had never smoked; a difference of 19.2%.
This suggests a relationship between the effect of smoking on perceived general health as age increased.
Table 5: Smoking Prevalence: by Age Group by Health, UK, January to December 2013
| % | ||||
| Age group | In good health | Not in good health | ||
| Current Smoker | Never Smoked | Current Smoker | Never Smoked | |
| 18-24 | 81.8 | 91.9 | 18.2 | 8.1 |
| 25-34 | 79.7 | 89.7 | 20.3 | 10.3 |
| 35-49 | 68.7 | 84.8 | 31.3 | 15.2 |
| 50-64 | 56.7 | 75.9 | 43.3 | 24.1 |
| 65+ | 47.8 | 60.6 | 52.2 | 39.4 |
| Source: Integrated Household Survey - Office for National Statistics | ||||
| Notes: | ||||
| 1. The total number of eligible responders to the question was 268,102. The question was asked to respondents aged 18 and over. | ||||
| 2. The health categories were split using the approach applied by Eurostat. 'In good health' contains the 'very good' and 'good' perceived health categories, and 'Not in good health' contains the categories 'fair', 'bad' and 'very bad'. | ||||
| 3. Percentages may not add to 100 per cent due to rounding. | ||||
| 4. Confidence intervals for the latest estimates in the above table are in the Excel download table. Information on what confidence intervals are is in the background notes. | ||||
Download this table Table 5: Smoking Prevalence: by Age Group by Health, UK, January to December 2013
.xls (29.7 kB)Notes for perceived general health and smoking prevalence
- This difference is based on unrounded estimates and maybe different to Table 5.